Increased “on-time” by 1.95 hours/day versus oral L-DOPA
49% Reduction in “off-time” vs oral L-DOPA (p<0.001)
Reduced dyskinesia
48% reduction in dyskinesia disability vs oral (p=0.002)
78% reduction in dyskinesia pain (p=0.02)
Approved by FDA, EMA, MHRA etc.
Marketed by AbbVie as Vyalev in USA, Produodopa in Europe
Analysts predict sales for continuous infusion of L-DOPA based products will reach $2 billion by 2030
Before continuous infusion
During continuous infusion
Continuous infusion - better control - but far from perfect
Still variable absorption depending on site, skin reactions and competitive transport across blood brain barrier.
Need to wear pump 24/7/365
Change infusion site every 1-2 days
High cost ($50K/year in USA)
Difficult for patients lacking dexterity
52% of patients give up within a year
MaavRx and better life for patients with advanced Parkinson's disease
How MaavRx works
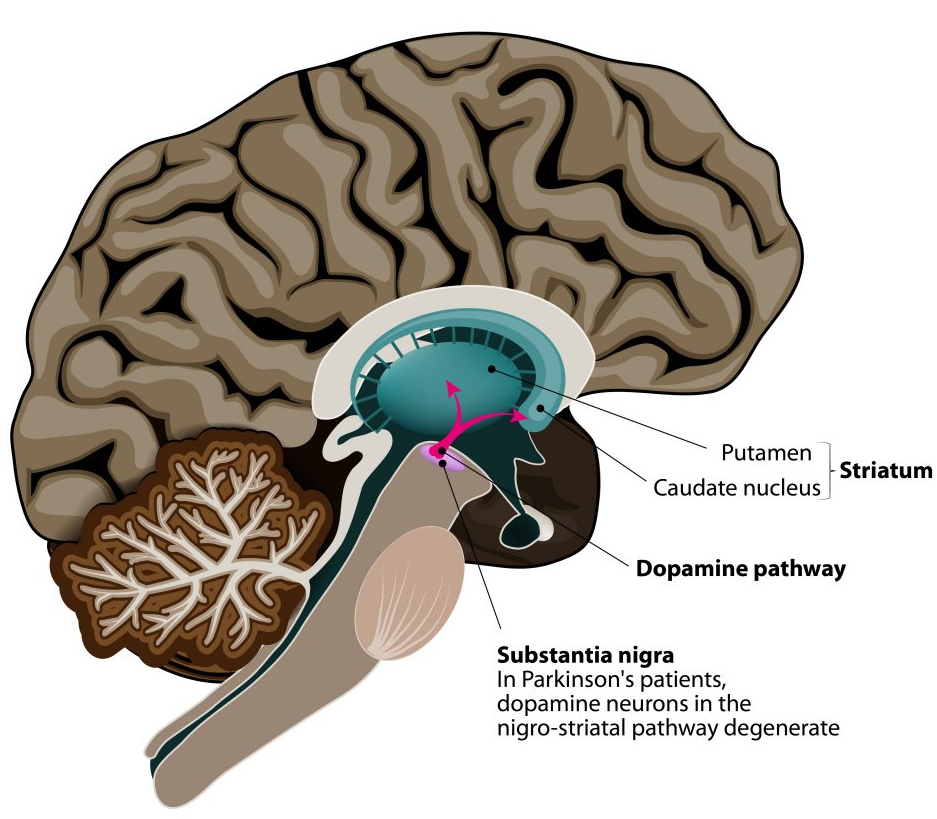
The motor symptoms of PD are due to the progressive loss of a cluster of cells supplying L-DOPA and dopamine to the brain putamen.
The neurons in the putamen remain healthy but do not function normally without L-DOPA
MaavRx uses proven AAV gene therapy technology to enable neurons in the putamen to make their own L-DOPA
We use an AAV5 vector to deliver the two genes (TH and GCH1) into the neurons.
Because these neurons survive for the lifetime of the patient, the benefit is expected to be lifelong
AAV5 vector particles deliver the genes to neurons in the putamen to enable them to produce constant non-fluctuation levels of L-DOPA
What are the expected advantages
One-time treatment for lifelong effect.
Constant levels of L-DOPA production for improved movement with no or reduced dyskinesia
No pump. No skin reactions.
Lower cost than continuous infusion.
What is the evidence MaavRx will work
Efficacy of prototype confirmed in classic (6OHDA) rat model of Parkinson’s disease.
Efficacy of prototype confirmed in classic (MPTP) primate model of disease.
Evidence that effect persist for 15 years in primate brain.
MaavRx AAV uses same vector, serotype, promoter and transgenes as prototype and with increase potency in vitro and strong expression throughout the putamen of large animals.
Preclinical proof of concept agreed by FDA – No need for further large animal efficacy studies
Single injection of 9E10 and 9E11 gene copies/animal cause significant continued improvement versus vehicle and low dose in primate model of PD. (Readministration of 9E10 also results in efficacy in animals previously treated with subtherapeutic dose)
What is the evidence MaavRx will be safe
Safety of prototype confirmed in GLP acute and chronic toxicology studies in rats and primates. No red flags.
No evidence of increased dyskinesia at highest doses in primate studies.
Similar technology using AAV vector to deliver a different gene into the same area of brain in children already approved by FDA and EMA (Upstaza for AADC deficiency)
Same technology using the same AAV serotype to deliver a different gene into the same area of brain confirmed to be well tolerated and effective in Huntington’s disease.
How easy is MaavRx to administer?
An outpatient MRI of the head is conducted to plan the infusion of MaavRx
MaavRx if infused locally via cannula into the right and left putamen.
Once the patient is prepared and positioned it takes about 10 minutes to insert the cannulas under local or general anaesthetic.
The patient is then moved to a recovery room and the infusion occurs while the patient is awake.
The cannulas are removed under local anaesthetic.
The patient goes home after overnight observation.
MaavRx Ltd plans to use Neurochase’s elegant cannula system to reduce cost and time for delivery
A greatly de-risked opportunity
Preclinical Safety and Efficacy
Dose related efficacy in multiple published studies in rat and primate models of PD
Expression persists for 15 years in primates
Well tolerated. No dyskinesia. No red flags on acute and chronic tox. studies in rats and primates
Low dose, local administration – avoids AAV high dose systemic toxicity
Relevant Human Data
Ample clinical data demonstrating the benefit of non-fluctuating L-DOPA
Same AAV serotype, also administered to the putamen in the same way: confirmed safe in patients (Huntington’s disease)
Regulatory and IP
Regulatory pathway and clinical study design defined by EMA/FDA approval of continuous subcutaneous L-DOPA prodrug.
Same AAV technology, same target (putamen), same delivery already approved by EMA/FDA (“Upstaza”)
Positive “Interact Meeting” with FDA
Approved patents USA and Europe
Commercial and Health Economics
Continuous subcutaneous infusion of L-DOPA at $50,000 / patient / year is reimbursed by US Insurers and UK NICE